
How India saved its mothers with Direct Cash Transfers
The Coronavirus pandemic has shown us how unaffordable health care in India is. In the last few months, patients have had to pay bills running in lakhs at private hospitals for Covid-19 treatment. There is no way ordinary Indians can afford that, and th..
By Upasha Kumari
The Coronavirus pandemic has shown us how unaffordable health care in India is. In the last few months, patients have had to pay bills running in lakhs at private hospitals for Covid-19 treatment. There is no way ordinary Indians can afford that, and that is the case for all quality healthcare services in India. Times like these make us wonder: how can public welfare schemes be used to improve access to healthcare?
During the initial months of the pandemic, when 70 per cent of the economic activities in the country came to a halt, the government resorted to a “Direct Cash Transfer” (DCT) mechanism to provide relief to over 800 million or two-thirds of India’s population. In fact, many economists have argued in favour of DCT as it is a means of providing immediate relief and confidence to the underprivileged people in an already economically and socially polarised society. Moreover, it is a sound economic policy measure as it encourages consumer spending and prevents the slowing down of the economy.
The Direct Cash Transfers mechanism involves a direct transfer of money to the bank account of the beneficiaries instead of offering them goods and services at subsidized prices. Policy experts prefer Direct Cash Transfers over subsidies because the latter is prone to failures such as improper targeting of beneficiaries, poor administrative capacity, corruption and leakages. Moreover, DCT expands the choice and freedom of the beneficiaries and they can avail any good or service of their choice from any seller or service provider in the market.
The benefits of Direct Cash Transfers are not limited only to the times of crisis; about 331 government schemes of the Indian government resort to DCT for improving public service delivery in the country.
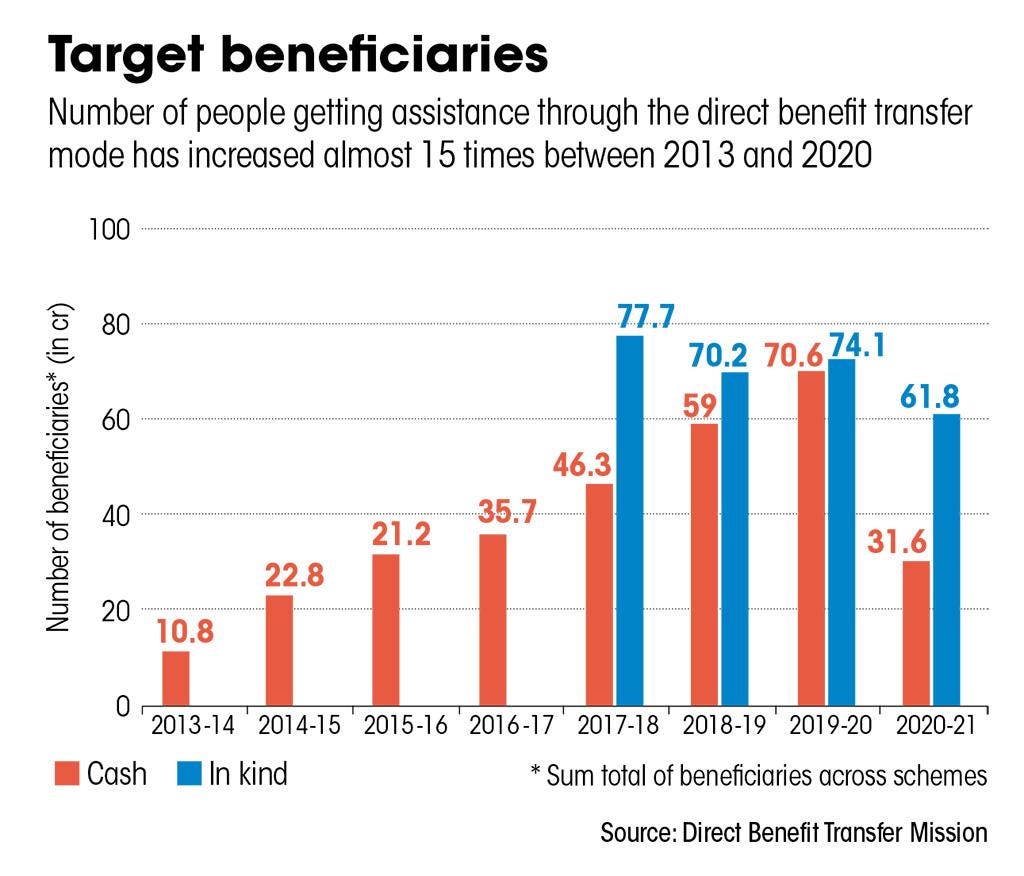
Figure 1: Target beneficiaries of DBT schemes from 2013-2021
Source: DownToEarth
The Pradhan Mantri Matru Vandana Yojana is an example of a Direct Cash Transfer scheme that has improved healthcare outcomes for India’s mothers. Let’s see how.
India’s Maternal Mortality Rate (MMR), or the number of maternal deaths per 1 lakh registered childbirths, has reduced over the last few years but it’s still double the targets set by the UN in their Sustainable Development Goals. One of the reasons for maternal deaths is the lack of institutionalised delivery, which means delivery that does not take place at a medical facility staffed by skilled delivery assistance, especially in rural areas.
Started from 1st January 2017, the Pradhan Mantri Matru Vandana Yojana (PMMVY) scheme [rechristened from the erstwhile Indira Gandhi Matritva Sahyog Yojana (IGMSY)], provides a cash incentive of Rs 5000 in three instalments to pregnant and lactating women aged 19 years or above for their first child. The first installment is given at the time of registration of pregnancy at the Anganwadi Center; the second installment is given after three months of delivery at the time of registration of childbirth and the third installment follows later. Further, an additional Rs 1000 is given to the woman under Janani Suraksha Yojana (JSY) after she avails institutional delivery of her child. By receiving the money directly in her account, the mother can access any of the three instalments from any location of the country. Thus, this scheme caters to the migrating class of people. Moreover, the mother can exercise her agency on how she wants to spend the money on herself and her child. Not only does this scheme aim at the financial empowerment of the woman but it also attends to her and the child’s health during and immediately after pregnancy.
The PMMVY scheme caters to the poor pregnant women living in states that have low institutional delivery rates, such as Uttar Pradesh, Uttarakhand, Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Assam, Rajasthan, Odisha and Jammu and Kashmir. The provisions of the scheme incentivize pregnant and lactating women to follow up their medical check-up from time to time even after the delivery of the child. Usually, expecting mothers from a poor socio-economic background neglect their prescribed medical checkups due to a lack of funds. According to the statistics presented by the Department of Women and Child Development in 2018, only 21% of the pregnant women attain full ante-natal checkups and 37 out of every 1000 infants born die within the first year of birth. Thus, the money being given under the scheme is crucial for those women who live in poverty. The scheme aims to reduce maternal and child mortality rate by attending to the needs of the pregnant women through routine medical checkup and improved nutritional intake. By receiving the money directly in her account, the woman can exercise her agency by deciding how she wants to spend the money on herself and her child. Not only does this scheme aim at the financial empowerment of the woman but it also attends to her and her child’s health during and immediately after pregnancy.
The efficiency in the implementation of the Scheme which was 38% in 2018 has touched the 90% mark in 2019. It is primarily due to the conditional cash transfer schemes of the government that the rate of institutional delivery has doubled from 38.7 to 79% during 2006-2016. (IGMSY was in force since 2010). As of February 2020, 1.28 crore beneficiaries received Direct Benefit Transfer under the PMMVY scheme directly in their bank accounts amounting to Rs. 5280 crore.
By devising more direct cash transfer schemes, not only can we improve the overall health of the marginalized communities but we can also significantly affect their health behaviour. Such schemes will encourage people to focus on preventive healthcare. Further, DCT improves financial inclusion, it encourages consumer spending, and it is likely to expand the choice and freedom of the individual. Implementing DCT in healthcare is a win-win situation for healthcare and the economy.
Read more: Loan Waivers Fail to Address Farmers’ Distress in India
About Upasha Kumari
Upasha has pursued her Bachelor's in Political Science from Lady Shri Ram College for Women, University of Delhi. She's currently a final year student at the Department of Political Science in the same university. Her key interest areas include development issues, public policy, gender, and Indian government and politics.